
Root canal treatment – when teeth lose their nerves
Root canal treatment is necessary to preserve the tooth if the dental pulp – also known as the dental nerve – inside the tooth is inflamed or dead. This is also referred to as ‘endodontic treatment’ and ‘endodontics’ or ‘endodontology’, because these treatments affect the endodont (the inside of the tooth). A specialist who performs root canal treatments is called an ‘endodontist’.
As our practice specialises in tooth preservation and endodontics, in this section we are providing a detailed overview of this important aspect of conservative dentistry. You can either download this comprehensive information in full as a PDF document, or read or print out sections on this website:
Overview of the topic:
- The dental nerve and its functions
- When the nerve is sick: how toothache develops
- Diagnostics: when is a tooth dead?
- When and why root canal treatment is necessary
- What is root canal treatment?
- How root canal treatment works
- Experience, success rate and complications of root canal treatments
- Children: performing root canal treatment on milk teeth
- Restoration (tooth reconstruction) after root canal treatment – pivot teeth
- How much does root canal treatment cost?
- Root canal treatment – questions and answers on the topic
The dental nerve and its functions
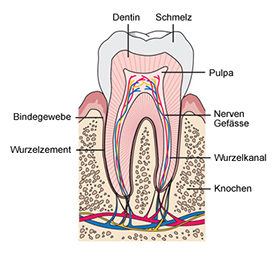
THE PULP – THE LIFELINE OF THE TOOTH
Inside the tooth is the pulp – often called the ‘nerve’ – whose soft tissue fills the root canals and the pulp cavity located in the crown of the tooth. The pulp is more than just the dental nerve, because in addition to nerve fibres it also contains blood vessels.
THE MOST IMPORTANT FUNCTIONS OF DENTAL PULP ARE:
Formation of hard tooth tissue
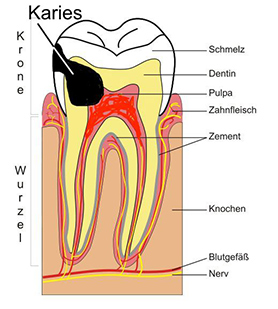
When teeth are formed in childhood and adolescence, the pulp cells produce the bone-like dentine, which makes up the majority of the hard tooth tissue. But even after teeth have erupted, the pulp continues to form dentine (secondary dentine), so the pulp cavity gradually becomes smaller throughout life. However, the pulp can also react to external stimuli, such as caries approaching the pulp or severe tooth wear. By building up a protective layer of dentine in the direction of the stimulus (tertiary dentine or stimulus dentine), the pulp attempts to ‘wall itself in’ and thus maintain its integrity and vitality.
Nutrition of the dentine
Like bone, dentine is a living substance that is connected to the pulp by means of the microscopic dentinal tubules. The cells and fluids in the tubules preserve the hard tooth tissue’s vitality and resilience.
Sensitivity
Sensory nerve fibres in the dentinal tubules ensure that the tooth is sensitive to chemical, thermal and mechanical stimuli, which explains why toothache can be caused by the likes of caries or drilling.
Defence
The tissue in the dentinal tubules also acts as a defence mechanism against microorganisms (such as bacteria) penetrating the tooth from the outside.
When the nerve is sick: how toothache develops

Like all living tissue, dental pulp can also be affected by pathological changes. This is usually inflammation of the pulp, which is known as ‘pulpitis’ and is categorised into acute and chronic forms. In the early stages, pulpitis is usually reversible (i.e. it be cured completely if the cause is eliminated). If the nerve is inflamed for an extended period of time, it is often irreversible. This means that it no longer heals and leads to chronic discomfort or ultimately to the death of the dental nerve (pulp necrosis)
Main causes of pulpitis:
- Caries (bacteria, which form toxins and acids)
- Cracks or fractures in the teeth (dental trauma)
- Chemical irritation caused by restorative dentistry such as fillings or crowns
- Overheating during dental treatment (e.g. when drilling or grinding the tooth without sufficient cooling)
Symptoms of pulpitis:
A typical symptom of pulpitis is pain, which may vary depending on the extent of the nerve inflammation.
- Hypersensitivity to cold or heat is often a sign of irritation or inflammation of the dental nerve. In this case, the pain is triggered by cold drinks or hot food. A persistently hypersensitive tooth neck can also be caused by chronic pulpitis. Hypersensitive teeth are often observed in the first few months after fillings or crowns have been inserted. Normally, the nerve calms down on its own. But if symptoms persist, root canal treatment may be necessary.
- Toothache is the classic symptom of pulpitis. When the dental nerve is acutely inflamed, the pain can occur in attacks and be very intense, often throbbing or pulsating. Sometimes, it radiates into the surrounding area (e.g. into the ear), which can make it difficult to localise the cause of the pain. Pulp toothache can occur spontaneously or be triggered by external influences such as temperature stimuli or biting. It is important to make a distinction between toothache due to other causes of pain that cause similar symptoms: headaches, pain in the temporomandibular joint, inflammation of the middle ear and trigeminal neuralgia. A heart attack can also occasionally cause pain radiating to the lower jaw.
- Pain when tapping and biting: If pulpitis persists for an extended period of time, the inflammation also affects the periodontal ligament and the bone around the tip of the root (apex). This is referred to as ‘acute apical periodontitis’ or ‘ostitis’. In this case, the toothache is load-dependent and occurs when biting down on something hard or tapping on the tooth, for example. As long as the dental nerve is vital (alive), the symptoms of pulpitis and apical periodontitis may overlap.
If the nerve dies (pulp necrosis)
If the dental pulp dies and the pulp tissue becomes necrotic, this is also referred to as ‘pulp necrosis’ or ‘gangrene’. The tooth is now described as devitalised (dead), because the dental nerve is no longer vital (living). Potential causes of pulp necrosis include:
Inflammation of the pulp (pulpitis) due to the likes of caries. Bacteria and their toxins can penetrate the pulp and cause it to die.
Dental trauma caused by an accident (e.g. a fall or blow) can also lead to pulp necrosis if the tooth is loosened or displaced and the blood vessels at the tip of the root are torn off.
Advanced periodontitis with very deep gum pockets can sometimes also lead to the death of the dental nerve (endo-perio lesion).
If the dental nerve dies following prolonged pulp inflammation (gangrene), the toothache often suddenly subsides because the nerve cells of the pulp are no longer transmitting pain stimuli. But, often, only the type of pain changes: from spontaneous pain to load-dependent pain that occurs when chewing, for example. This is due to the bacteria that now colonise the dead pulp tissue and penetrate the neighbouring bone via the tip of the root (the technical term for this is ‘apical ostitis’ or ‘apical periodontitis’).
From the dead tooth to the ‘swollen jaw’

The bacteria from the ‘dead tooth root’ now penetrate the bone via the tip of the root, causing localised bone inflammation (ostitis) and slow degradation of the bone. This can be completely painless, so many dead teeth are only discovered by chance when an X-ray is taken.
In some cases, however, the inflammation is more acute, the affected tooth looks ‘longer’ and hurts when it is loaded (when biting). Feeling like a tooth is elongated is due to the fact that the tooth, which is anchored in the bone with elastic fibres, is pushed out of the tooth socket by fractions of a millimetre by the inflammation, and it hits the opposing tooth earlier when biting.
The bone around the ‘dead’ root is attacked and slowly degraded by the bacteria and, after some time, a black ‘shadow’ the size of a lentil or pea can often be seen at the tip of the root on an X-ray. Depending on how aggressive the bacteria is and on the immune system’s defences, this ostitis can remain stable for a long time. If the bacteria gain the upper hand, the inflammation spreads further in the bone and can break through into the soft tissue. After experiencing severe pain initially, the patient then notices that their lip, cheek or chin is becoming increasingly swollen. If pus accumulates in the tissue, this is known as an abscess (boil). This ‘swollen jaw’ is not harmless by any means and must be treated immediately. An untreated abscess in the facial area can even have life-threatening consequences.
Diagnostics: when is a tooth dead?
1. TAPPING OR PERCUSSION TEST
Carefully tapping the tooth in question with an instrument can give initial indications as to its vitality. If the tooth is devitalised (dead), the patient often feels an unpleasant sensation or slight pain. This test can also be carried out as a bite test with a small cotton roller that the patient bites on with the tooth.
2. VITALITY TEST
During the cold test, the tooth’s sensitivity is tested with CO2 snow (at a temperature of -78°C). If the pulp is vital, a strong cold stimulus is normally felt. If in doubt, an electric pulp tester may also be helpful. It emits electricity and triggers a tingling sensation in the tooth if the pulp is vital. These vitality tests are not always reliable and sometimes do not allow a definitive statement to be made with respect to a tooth’s vitality. In teeth with multiple roots, for example, the pulp of one root may already be dead while the other roots are still vital and sensitive. Sometimes, even a vital tooth does not react to the test because the pulp has receded considerably and has been ‘walled in’ by the formation of hard tissue. A ceramic crown can also make it difficult to assess vitality.
3. X-RAY IMAGING
X-rays provide the dental practitioner with valuable information for assessing a tooth prior to performing any root canal treatment. A widened periodontal gap in the transition between the root of the tooth and the bone may be an indication of inflammation spreading in dead dental pulp. If the bone around the tip of the root has already degraded in the X-ray image, this will show up as a roundish black shadow. The inflammatory tissue located there, which attacks the bone, is also known as a ‘granuloma’. However, dead teeth can also cause cysts. Dental granulomas and cysts indicate that the dental pulp is dead (i.e. the tooth is devitalised). Root canal treatment should not be delayed in such cases.
In rare cases, especially if both the anatomy of the root and the symptoms are unclear, a 3D X-ray (DVT) may also be necessary. Such computer tomography provides three-dimensional images and allows a very precise diagnosis of the roots of the tooth and the surrounding hard and soft tissue. Our practice has a latest-generation digital volume tomograph, which guarantees particularly low exposure to radiation.
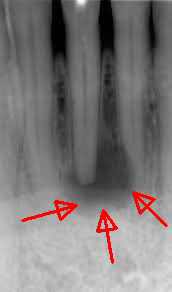
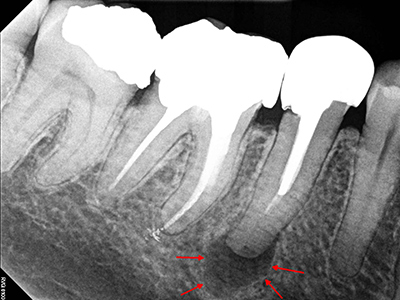
Dead lower incisor in the X-ray image. The patient did not feel any pain whatsoever. The dark zone around the tip of the root shows the degradation of the bone due to the inflammation, which is also referred to as a ‘granuloma’ or ‘apical ostitis’. Root canal treatment is urgently needed to prevent major damage such as a fistula or an abscess.

Despite root canal treatment, this patient had persistent, chronic discomfort in the top-right first molar (M-tooth). There was nothing remarkable on the normal X-ray. Only the 3D volume tomography shows an unfilled additional canal in the anterior root. The pain subsided immediately after revising and filling this canal.
When and why root canal treatment is necessary
- If the dental pulp is irreversibly inflamed (pulpitis) and persistent or constantly recurring toothache occurs. The pain, which the patient often finds unbearable, can only be permanently eliminated by means of root canal treatment.
- If the dental nerve is completely or partially dead (pulp necrosis, gangrene). A devitalised (dead) tooth requires root canal treatment to prevent bacteria from colonising the inside of the tooth.
What is root canal treatment?
During root canal treatment (also known by the technical term ‘endodontic treatment’), the tooth’s ‘nerve is pulled out’. The pulp tissue is completely removed from the inside of the tooth, and the root of the tooth and the root canal(s) are sealed are tightly as possible by filling the roots. The dentist must have good knowledge of the anatomical structure of the root of the tooth and know how many roots and canals the tooth has. The number of roots and canals per root varies a great deal. For example, a top first premolar can have one or two roots and between one and three root canals. So the dentist must always check in each individual case how many root canals are actually present, so they can ensure that all the canals are treated completely. The use of X-ray images and magnification aids during work is indispensable for this.
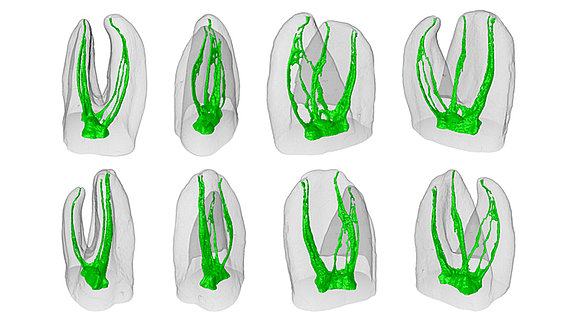
Visualisation of the root canals in molars (M-teeth): the number, branches and course of the canals vary a great deal. As a result, root canal treatments for these teeth can sometimes be very complicated. Occasionally, it is technically impossible to completely prepare and fill all of the canals and branches (side canals).
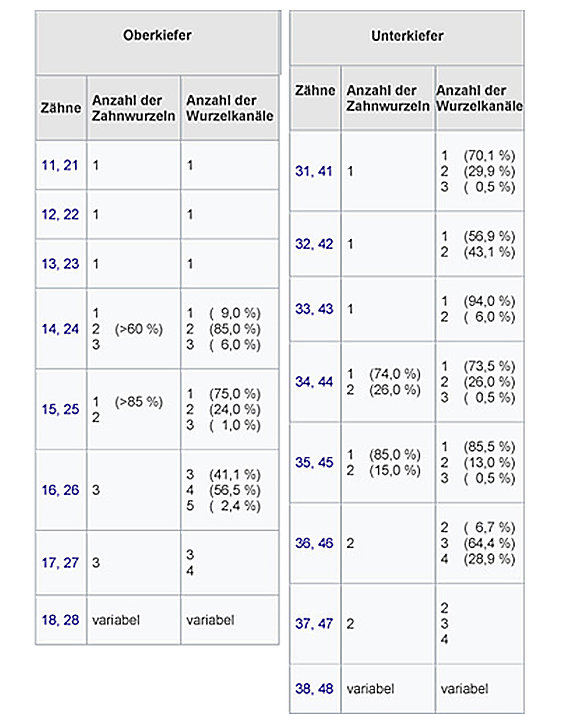
The number of roots and canals per tooth can vary a great deal, as shown in the table
How root canal treatment works
1. ANAESTHETISATION
The tooth to be treated is locally anaesthetised using a local anaesthetic if the nerve is still vital (the tooth is still living). With the correct anaesthetic, root canal treatment is absolutely painless. If teeth are devitalised (dead), there is often no need for anaesthesia. We also offer anxious patients nitrous oxide sedation to help them relax.
2. ISOLATION

A thin, perforated rubber film (elasticated rubber, rubber dam) is pulled over the tooth and secured with clamps. This isolates the tooth from the oral cavity and prevents saliva and bacteria from the mouth from entering the root canal. At the same time, the elasticated rubber prevents the needle-shaped root canal instruments from accidentally falling into the mouth during root canal treatment (when there is a risk of swallowing or inhalation).
3. DRILLING THE TOOTH (TREPANATION)
The tooth is now drilled (trepanned) from above (occlusal surface) or behind (incisors and canines) to open the pulp cavity and create free access to the root canals. The dental practitioner now searches for the entrances to the root canals at the bottom of the pulp cavity. It is extremely important to use optical magnification (magnifying glasses or a microscope) during this process.
4. VISUALISING THE ENTRANCES TO THE ROOT CANALS – WORKING WITH THE MICROSCOPE
Performing root canal treatments involves high-precision work with extremely fine, fragile instruments in a dark space that is difficult to see and often only fractions of a millimetre in size. Good vision is crucial for successful treatment, which is why a growing number of endodontic specialists use a microscope for root canal treatments. A modern Zeiss dental microscope is available in our practice for endodontic procedures. Anatomical structures and problems that are otherwise often overlooked can be visualised thanks to the magnification and perfect illumination of the working area.
- Additional root canals:
Many failed root canal treatments are due to the fact that not all of the root canals are found and filled. Untreated root canals can then lead to chronic inflammation and pain. Under the microscope, the chances of detecting even hidden canal entrances and tightly filling all of the root canals are optimised. - Cracked teeth:
Chronic toothache can sometimes also be caused by microcracks in the tooth. If cracked teeth go undetected, the pain can persist despite root canal treatment apparently being successful. The microscope enables diagnosis of microcracks in teeth that would otherwise usually go undetected and therefore help to avoid lengthy and expensive unnecessary treatment. - Broken root canal instruments:
The very thin, fragile files used to prepare and widen the root canals can occasionally break off in the canal, especially if it is very curved. Fortunately, experienced endodontic specialists can remove the fragments from the root canal in many cases. The microscope provides valuable assistance here. - Perforations:
Another potential complication of root canal treatment is perforation. When exposing or widening the root canals, the wall of the tooth is pushed outwards. Such perforations can be successfully sealed with special cements, and the tooth can be preserved. The microscope is extremely helpful when sealing a perforation.
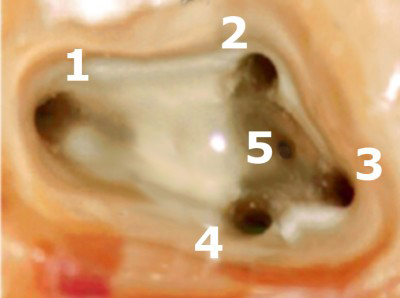
Visualising the entrances to the canals under the microscope. Thanks to the magnification, five canals were found and prepared in this molar (back tooth). The entrances are first of all carefully widened in a funnel shape using appropriate instruments, so that the root canal instruments can be inserted more easily.
5. MEASURING THE LENGTH
Before preparing the root canals, the dental practitioner must determine how long they are. This is the only way to prepare the canal right up to the tip of the root (apex). The X-ray taken before the root canal treatment gives an initial indication of the approximate root length. A precise measurement (endometry) is then carried out with the electronic length measuring device, which indicates the exact distance to the tip of the root (apex) when the root canal instrument is inserted. If in doubt, it may be useful to perform an additional X-ray measurement with visualisation of the canal files inserted previously. In our practice, we only use digital X-ray images with high resolution, fast availability and a very low radiation dose.

Electronic measuring device for determining the length of root canals
6. PREPARING THE ROOT CANALS
The root canals are now gently widened using a series of special, coordinated and needle-shaped instruments. In addition to the file-like handheld instruments, high-elasticity rotating root canal instruments are used nowadays. They are usually made of a nickel-titanium (Ni-Ti) alloy and can follow even curved root canals safely to the tip. Propulsion is provided by an electronically controlled micromotor with a precisely defined torque, so that the delicate files do not break off in the canal. In our practice, we use ProTaper Next® root canal instruments, which have been proven to prepare the canal particularly quickly and safely. To further minimise the risk of the canal instruments breaking (fracturing), we only use them as single-use instruments.
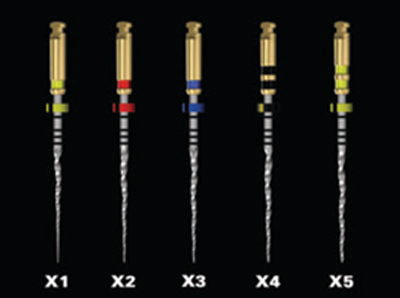
The extremely flexible root canal instruments in the Pro Taper Next® series guarantee efficient and safe canal preparation.
7. CLEANING AND DISINFECTING THE ROOT CANAL
After each instrument is used, the canal is rinsed with a disinfectant liquid (sodium hypochlorite). Once preparation is complete, the canal is dried with sterile paper tips.
8. MEDICATING THE CANAL
This intermediate step is only necessary if the root canal was infected and/or the treated tooth was causing the patient pain. In this case, a disinfectant paste is applied to the root canal first of all and the tooth is sealed with a temporary filling. The root canal is filled a few days later.
9. FILLING THE ROOT CANALS
The cleaned, disinfected and dried root canals are now sealed as tightly as possible up to the tip of the root with a root filling. For this purpose, a viscous cement (sealer) and pins made of gutta-percha are inserted into the canal. The gutta-percha can also be compressed (condensation) with special instruments (pluggers) or softened with heat (thermoplastic root canal filling) to seal the branches of the root canals (‘side canals’) as well as possible.
10. SEALING THE TOOTH AND TAKING AN X-RAY
Once the root canal is filled, the tooth is sealed from above with a plastic filling (composite) to make it bacteria-proof. Hermetic sealing is very important, as otherwise the root canal will be recolonised by bacteria from the oral cavity. An control X-ray image documents the root filling at the end.

The control X-ray image after root canal treatment of teeth 16 and 15 shows root canals correctly filled up to the tip of the root (apex) (four canals in tooth 16, two canals in tooth 15)
This video (in English) shows the process of a root canal treatment
Experience, success rate and complications of root canal treatments
Endodontic treatments are performed in confined, hard-to-reach spaces and are technically challenging. So successful treatment depends largely on practice and the skill of the practitioner. The use of visual aids such as magnifying glasses or microscopes and modern root canal instruments can improve the success rate of root canal treatment. If these conditions are met, experience suggests a success rate of 70 – 90%.
But there can still sometimes be problems and complications that can thwart successful endodontic treatment:
- Not all of the root canals are found / filled: The number of root canals varies a great deal. A first molar (back tooth) can have two, three, four or even five root canals. If not all of the canals are filled during root canal treatment, this can lead to permanent pain or the development of chronic bacterial inflammation at the tip of the root (granulomas). The use of magnifying visual aids (magnifying glasses or a microscope) is particularly helpful for locating the canals.
- The root canals are not prepared / filled up to the tip of the root (underfilling): It is often difficult to prepare and fill the canals up to the tip of the root (apex), particularly when roots are severely curved and root canals are calcified. A root filling that is too short (underfilling) can lead to bacteria colonising the unfilled part of the root and to chronic bone inflammation (apical ostitis).
- The root canals are prepared / filled beyond the tip of the root (overfilling): Cement (sealer) or gutta-percha gets into the bone and can cause problems there, such as acute or chronic foreign body inflammation. It is particularly critical if root filling material gets into the maxillary sinus or the nerve canal in the lower jaw. Sometimes the tip of the root needs to be surgically removed (apicoectomy) to remove the foreign body.

Root filling too long (overfilling): Root filling cement and gutta-percha were pressed into the bone beyond the tip of the root. If the material penetrates the nerve canal of the lower jaw, this can lead to permanent damage to the sensory nerves of the lower lip.
- The root canal is perforated during preparation: Particularly when root canals are curved, the canal wall may be pierced and perforated outwards during preparation (via falsa). Such perforations can be closed in some cases, but can also lead to tooth loss.
- The root canal instrument breaks off in the canal (fracture): In narrow and curved root canals, the delicate rotating preparation instruments have to withstand enormous loads. If the instrument breaks (fractures), it is usually difficult to remove the fragment stuck in the canal. Removal can be successful with the help of special instruments and visual aids (microscope). Otherwise, an apicoectomy can help in some cases if the broken instrument is close to the tip of the root. If the fragment cannot be removed from the canal, there is a risk of bacterial colonisation and bone inflammation at the tip of the root. To avoid such instrument breakages as far as possible, we only use our root canal instruments once and then dispose of them. Also, we only use rotating instruments with a torque-controlled micromotor that automatically reverses the rotary movement if a defined load is exceeded.
- The treated tooth is not sealed against bacteria: If the filling or crown made after root canal treatment is not completely sealed and impermeable to bacteria, microorganisms will recontaminate the root filling over time, penetrating it from the mouth and colonising it. This is a common cause of what is known as ‘recurrence’ (failure of root canal treatment), in which the inflammatory symptoms recur after a certain period of time.
Children: performing root canal treatment on milk teeth
Premature loss of milk teeth can have harmful consequences for permanent teeth. So, in some cases, it may be advisable to carry out root canal treatment to preserve decayed milk teeth. With local anaesthesia, these treatments are completely painless. Anxious children can be treated with nitrous oxide or, if necessary, under general anaesthetic.
If the dental nerve is not yet inflamed, it is sometimes sufficient to only remove the upper part (the crown pulp). The root pulp is then covered and remains vital. This procedure is known as a ‘pulpotomy’ or ‘vital amputation’. If the pulp is already inflamed, a milk tooth root filling may be indicated in some cases. However, a resorbable root filling material that can be biodegraded when the milk tooth root dissolves during tooth replacement must be used for milk teeth. After root canal treatment, the milk tooth must be restored with a special milk tooth crown so that it does not break off. Root canal treatments performed on milk teeth are difficult and should only be carried out by experienced practitioners. In addition to their qualifications in paediatric dentistry, our paediatric dentists have also completed further training in endodontics. Click here for more information about paediatric dentistry.
Restoration (tooth reconstruction) after root canal treatment – pivot teeth
The tooth that has undergone root canal treatment is first of all treated with a tightly sealed reconstructive filling to prevent bacteria from penetrating. The tooth is mechanically weakened after root canal treatment, and there is a risk that it will break off (fracture) sooner or later, especially if it is one of the back teeth. For this reason, posterior teeth (premolars and molars) that undergo root canal treatment are often restored with a crown to protect them from fractures.
If the tooth that undergoes root canal treatment is severely damaged by caries, it sometimes has to be stabilised with a post and core. A root canal post made of glass fibre, metal or zirconium ceramic is bonded (cemented) into the root canal. The stump is then built up with composite and restored with a crown. Such cases are also referred to as ‘pivot teeth’ or ‘pivot crowns’. A pivot tooth is no longer used as often nowadays, as root canal posts can also cause cracks or fractures in the root of the tooth. If the root’s prognosis is poor, replacing the tooth with an implant is usually preferable to a pivot tooth.
Front teeth (incisors, canines) are subject to less mechanical stress and generally do not need to be crowned after root canal treatment. However, dark discolouration sometimes occurs after the root canal filling. This can be aesthetically unpleasant in front teeth. Internal bleaching can remedy this. Sometimes, for aesthetic reasons, a ceramic veneer or a crown is necessary to permanently conceal the dark discolouration.
How much does root canal treatment cost?
The cost of root canal treatment depends primarily on the number of canals treated.
Depending on the number of root canals, the costs usually range from CHF 700 to CHF 2,200 per tooth. The use of a microscope may incur additional costs.
Root canal treatments – questions and answers on the topic
Yes. Root canal treatment is absolutely necessary if you have dead teeth. Otherwise, the root canals of dead teeth are colonised by bacteria and the bone can become inflamed. These inflammations are often completely painless at first and usually go unnoticed.
No. The pain can be completely eliminated by administering a local anaesthetic. Nevertheless, many patients find the often lengthy and complex root canal treatments stressful. That is why, in addition to local anaesthesia, we offer sedation with nitrous oxide or twilight sleep dentistry with sedatives on request. This allows our patients to completely relax during treatment.
Yes. That is possible. However, it is usually not the tooth that hurts, but rather the bone around the tip of the root. In the first few weeks after root canal treatment, the tissue there is still irritated and can hurt when you put pressure on it (biting). These initial symptoms generally disappear over time. In some cases, especially in the case of teeth with several roots, root canals are ‘overlooked’ by the dentist and are not filled or are not filled correctly, which then leads to inflammation and pain. It is then necessary to repeat (revise) the root canal filling, so that all of the canals can be properly filled up to the tip of the root.
If the root canals are not infected, the entire root canal treatment can be completed in a single session. If the patient has toothache and the root canal is infected, the root canal is usually filled with a disinfectant medication first of all, and the actual process of filling the root canal is carried out later in a second step.
Yes. In most cases, this is possible. This is referred to as a ‘revision’. The old root canal filling must be completely removed from the canals first of all, before a new tight root canal filling can be placed. Special care must be taken during revisions, as there is always a risk of perforating the root canal. It becomes particularly difficult if the canal is blocked by root canal posts and cores. Sometimes, surgically removing the tip of the root (tip of the root resection) is an alternative to revision.
If root canal treatment is carried out carefully and correctly, the long-term prognosis is very good. Such teeth can work well for a lifetime. We know from experience that teeth that have undergone root canal treatment and are subject to heavy chewing stress should be crowned to prevent them from breaking.
In most cases, the granuloma or apical ostitis recedes and heals after root canal treatment. However, a cyst can still continue to grow, which is why an X-ray check-up after several months is important. If the cyst or granuloma has not become smaller or disappeared entirely, it must be surgically removed (apicoectomy).
From a medical point of view, a tooth that has a correctly placed root canal filling and that is showing no signs of inflammation is not an interference field and should not be removed on this basis under any circumstances.