Dental Braces for Children

Introduction
Fortunately not all children require a dental brace. Children should be examined by an orthodontist to determine whether and when treatment is required.
When should the examination take place?
- First examination at 4 years (milk teeth)
- Second examination at 8 years (early transitional dentition)
- Third examination at 12 years (late transitional dentition)
When should treatment begin?
Generally treatment begins between the ages of 7 and 12. An earlier start to treatment in the deciduous dentition is only required in difficult cases.
Removable orthodontic apparatus (expansion plate)
Removable dental braces are the standard tooth correction appliances for children and young adults. The appliance uses the natural growth of the jaws during this period to guide the teeth and bony structures gently into the correct position. There are various types of removable appliances for different areas of application, e.g. orthodontic expansion plates, activators and bionators. They all have one thing in common; they must be worn regularly for about 15 hours a day to produce good results. A check-up is required about every 4 weeks with the orthodontist; if required the expansion screws in the appliance are then reactivated to maintain the pressure on the teeth and jaws.
Important:
- Success depends on wearing the appliance regularly! This means that parents have to keep their children motivated.
- Do not wear removable appliances when eating and always keep the teeth and dental braces clean to prevent caries!
- When the brace is not in use, it should be kept in a sturdy box to ensure it is not accidentally damaged or lost.
Fixed dental braces

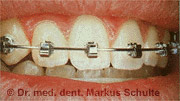
Removable dental braces cannot be used in complex cases with severe malalignment of the teeth and jaw bones. In these cases modern orthodontics increasingly uses fixed appliances, also known as multi-band appliances, for children and young adults: small attachments called brackets made from metal, plastic or porcelain are bonded to the teeth with adhesive and connected with custom bent flexible wire arches, which are changed at regular intervals. The force applied by the arches moves the teeth very precisely into the required position. Tooth correction with fixed dental braces is generally completed in 2 – 3 years and therefore requires less time on average than treatment with a removable appliance.
Treatment does not depend on the discipline of the child or parents, as the appliance functions 24 hours a day. Fixed dental braces are effective regardless of age – they function just as well for adults as for children.


Before and after multi-band treatment in the upper and lower jaw
One disadvantage is that fixed appliances with brackets and arches make it difficult to clean the teeth, increasing the risk of caries. Particularly thorough and precise oral hygiene with special toothbrushes is therefore required. Our dental hygienists provide special instructions for dental brace wearers. Not every patient is comfortable with the “silver smile” of a fixed dental brace, though the aesthetics of dental braces has been improved in the past few years: transparent brackets made from porcelain or plastic are hardly visible. The latest type uses the lingual technique to bond the appliance onto the inner surface of the teeth and is therefore completely invisible. Further details can be found at Adult treatment.

Preventing a relapse: After correction, teeth have a tendency to return to their original position. The risk of relapse used to be underestimated. Consequently, after spending a lot of time and effort obtaining initially good results, many patients (and orthodontists) felt frustrated that the teeth returned to their original malposition over several years.
This problem is now solved by fitting a retainer after completion of treatment, which fixes the teeth in their new position. A thin wire, which is bonded with adhesive onto the inner surfaces of the teeth and remains fitted for many years, is generally used as a retainer.
treatment time by up to 50%
thanks to better power
transmission, minimal
irritation of the lips and cheek
due to the small size, better
aesthetics and hygiene.
Prevent relapse: After a tooth correction, the teeth have a tendency to return to their old position. In earlier times, this risk of relapse was underestimated. Therefore, many patients (and orthodontists) had the frustrating experience that after a long and painstaking dental correction with initially good results, the teeth wandered back to the old faulty position over several years.
Today, this problem is solved by the use of a so-called Retainer , which fixes the teeth in their new position. It usually uses a thin wire, which is glued to the inside of the teeth and remains there for many years. Alternatively, a removable retainer rail can be used, which is worn only at night.

Prophylaxis: Parents′ responsibilities

About half of tooth and jaw anomalies are not inherited or congenital, but are acquired through bad habits, e.g. thumb sucking, or due to the premature loss of milk teeth.
Prolonged thumb sucking can cause the anterior section of the upper jaw including the incisal teeth to protrude. At the same time the lower jaw is pushed back. The result is an open bite due to thumb sucking, in which the incisal teeth can no longer be closed. This can also cause speech defects and mouth breathing.
All small children need something to suck on. It is much better for the child to suck a dummy rather than a thumb. From an orthodontic point of view there is nothing wrong with moderate use of a dummy up to the age of three.
Milk teeth have an important function as space maintainers, i.e. they keep the correct amount of space free for the permanent teeth. Premature loss of the posterior milk teeth due to caries can therefore cause severe malocclusion in the permanent dentition. Optimum oral hygiene from early childhood and healthy nutrition are therefore important for maintaining the milk teeth until eruption of the permanent teeth.
Our paediatric dentist is happy to offer advice on orthodontic prophylaxis.

